Orthopedic billing denials rarely happen because of clinical mistakes. Most revenue loss comes from preventable billing and coding gaps that surface later as denials, delays, or underpayments.
Common issues like missing prior authorization, incorrect modifiers, global period conflicts, laterality errors (RT/LT), and weak documentation can quickly disrupt reimbursement even when clinical care is accurate.
The impact is significant:
- Slower cash flow despite a full schedule
- Increased administrative rework and appeals
- Rising A/R aging beyond 60–90 days
Because orthopedic revenue depends heavily on surgeries, imaging, injections, and DME, even small billing errors can lead to major revenue leakage. This guide breaks down the most common reasons for orthopedic billing denials and how to fix them at the source to improve clean-claim performance.
What Is an Orthopedic Billing Denial? (And How It Differs From a Rejection)
In orthopedic billing, a denial means the payer accepted the claim into its adjudication workflow, reviewed it against coverage and policy rules, and then issued a non-payment or partial payment. Common denial triggers include authorization issues, modifier errors, medical-necessity issues, global-period conflicts, and incomplete documentation.
A rejection happens earlier in the claim lifecycle. Instead of being formally processed by the payer, the claim fails front-end edits and is returned before adjudication. Rejections are usually caused by incorrect patient information, NPI or taxonomy mismatches, missing claim fields, invalid coding combinations, or place-of-service errors.
The distinction matters because each issue requires a different response.
Rejections are typically clean-claim problems that require correction and fast resubmission. Denials, however, require deeper revenue cycle review, including coding analysis, documentation support, or formal appeals.
For orthopedic practices where reimbursement depends heavily on high-value procedures, treating denials like “just another resubmission” is how A/R stretches into 60–90+ day territory.
Common Orthopedic Billing Denial Categories That Delay Reimbursement
Most orthopedic billing denials fall into four major categories. Identifying denials by root cause helps practices reduce repeat claim issues, improve clean-claim rates, and strengthen overall revenue cycle performance.
1. Eligibility, Benefits, and Coverage Denials
These denials occur when the payer’s records do not match what was assumed during scheduling or patient check-in. Even when coverage appears active, the specific orthopedic service may still be limited by network rules, referral requirements, therapy caps, imaging restrictions, or plan exclusions.
2. Prior Authorization and Referral Denials
Orthopedic services such as surgeries, injections, MRIs, DME, and physical therapy frequently require payer authorization before treatment. Claims are commonly denied when the authorization is missing, expired, or mismatched to the CPT code, facility, or date of service.
3. Coding, Modifier, and Bundling Denials
Orthopedic coding denials are often caused by NCCI edits, modifier misuse, laterality mismatches, wrong units, unsupported add-on codes, or incorrect assistant surgeon billing logic. Because orthopedic reimbursement is highly modifier-dependent, even a small coding mistake can trigger reduced payment or full denial.
4. Documentation and Medical Necessity Denials
Orthopedic billing is heavily documentation-driven. Payers often request records to validate symptom severity, functional limitations, imaging findings, conservative treatment history, and procedure rationale. Weak documentation doesn’t just increase denials; it can also create audit and recoupment risks later.
Orthopedic Claim Denial Trends: Where Revenue Leakage Usually Starts
Most orthopedic denials are not isolated incidents. They are recurring workflow failures that quietly disrupt reimbursement over time. A missing authorization, incorrect modifier, documentation gap, or eligibility mismatch may seem minor individually, but repeated claim issues can quickly slow collections and increase A/R aging.
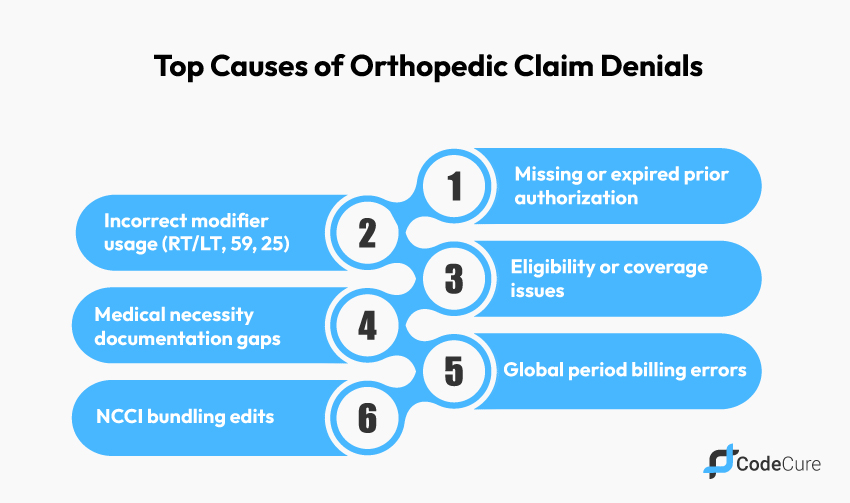
The most common denial patterns in orthopedic billing typically involve:
- Prior authorization mismatches
- Modifier and laterality errors
- Medical necessity documentation gaps
- Global period billing conflicts
- Enrollment and credentialing inconsistencies
Practices that identify these trends early are far more successful at improving clean-claim rates and reducing repeat denials.
15 Most Common Orthopedic Billing Denials (With Proven Fixes That Reduce Rejections)
Below are the most common orthopedic billing denial reasons affecting practices today and the operational fixes that help reduce repeat claim denials.
1. Orthopedic Insurance Eligibility Verification Errors Leading to Claim Denials
Eligibility denials are one of the most common orthopedic claim issues because many practices verify only whether the patient is “active” without confirming whether the actual orthopedic service is covered.
Problems often arise when the patient’s plan includes referral requirements, therapy limitations, network restrictions, or imaging exclusions.
To reduce these denials, orthopedic practices should verify eligibility before the appointment and reconfirm coverage for surgeries, MRIs, injections, and other high-cost procedures on the date of service.
2. Missing or Expired Prior Authorization for Orthopedic Procedures
Prior authorization denials are a major challenge in orthopedic billing because many services require payer approval before treatment.
Procedures such as surgeries, spinal injections, MRIs, DME, and physical therapy are frequently subject to authorization requirements. Claims are commonly denied when the authorization has expired, is linked to the wrong CPT code, or is mismatched to the facility or date of service.
Maintaining a detailed authorization tracking process and validating approvals before claim submission can significantly reduce these denials.
3. Referral and PCP Mismatch Denials in Orthopedic Claims
Orthopedic practices working with HMO and managed care plans often face denials related to missing referrals or PCP mismatches.
These denials occur when the referral is inactive, assigned to the wrong provider, or missing entirely from the payer’s system. Strong front-end verification processes help reduce these issues before the patient is seen.
Scheduling teams should verify referral requirements early and confirm that referral information matches payer records before claims are submitted.
4. Medical Necessity Denials for Orthopedic Services
Medical necessity denials happen when the payer believes the diagnosis does not support the orthopedic procedure billed.
These denials are especially common for surgeries, injections, imaging, and advanced orthopedic treatments. Payers often review symptom severity, functional limitations, imaging findings, and conservative treatment history before approving reimbursement.
Clear documentation connecting the diagnosis, clinical findings, and treatment rationale is essential for preventing these denials.
5. RT/LT Laterality Errors in Orthopedic Billing
Laterality mistakes are one of the easiest orthopedic billing errors for payers to identify.
Claims are frequently denied when documentation, imaging reports, operative notes, and billing modifiers do not consistently identify the same anatomical side. Even a small inconsistency between the chart and claim can delay payment.
Orthopedic practices can reduce these denials by standardizing laterality documentation across clinical, coding, and billing workflows.
6. Incorrect Modifier Usage in Orthopedic Coding
Modifier-related denials are among the most expensive orthopedic coding problems because reimbursement often depends on accurate modifier selection.
Missing modifiers, invalid modifier combinations, or payer-specific coding edits can quickly turn a payable claim into a denial. Since orthopedic procedures frequently involve bilateral services, multiple procedures, and E/M visits with procedures, coding teams should use specialty-specific coding review processes before submission.
7. Modifier Documentation Errors in Orthopedic Billing
Even when the correct modifier is billed, orthopedic claims may still be denied if the documentation does not clearly support the coding scenario.
Distinct procedural service modifiers, for example, require detailed documentation proving the procedures were separate and independently billable. Strong operative documentation should clearly explain separate anatomical sites, procedures, or clinical circumstances whenever modifiers are used to bypass payer edits.
8. NCCI Bundling Denials in Orthopedic Surgery Billing
Bundling denials occur when payers determine that one orthopedic procedure should be included within another billed service under NCCI edit guidelines.
These denials are especially common in orthopedic surgery and multi-procedure encounters. Orthopedic billing teams should validate modifier usage carefully and ensure documentation fully supports any separately billable procedures before claim submission.
| Denial Type | Common Cause | Prevention Strategy |
| Prior Authorization | Missing or mismatched authorization | Pre-submission authorization review |
| Modifier Errors | Incorrect RT/LT or modifier usage | Orthopedic coding QA workflows |
| Global Period Denials | Post-op billing conflicts | Surgical package verification |
| Medical Necessity | Weak documentation support | Clinical documentation audits |
9. Global Period Billing Denials for Post-Operative Visits
Global period denials happen when follow-up visits or additional services are billed separately, even though they are included in the surgical package.
These denials are common in orthopedic practices with high surgical volume. Before billing post-operative services, teams should verify global period status and determine whether the visit qualifies for separate reimbursement.
Documentation should clearly support unrelated conditions or separately billable medical decision-making when applicable.
10. Duplicate Claim Submission Errors in Orthopedic Billing
Duplicate claim denials often occur when practices resubmit claims too quickly without checking payer acknowledgement or claim status.
These unnecessary resubmissions create confusion, delay reimbursement, and increase administrative workload. Tracking claim activity carefully and using corrected-claim indicators properly can help avoid duplicate billing issues.
11. Timely Filing Denials in Orthopedic Billing
Timely filing denials happen when claims or appeals are submitted after the payer’s filing deadline.
These denials are entirely preventable but can still lead to significant revenue loss. Orthopedic practices should establish strict claim submission timelines and work denials consistently instead of waiting until A/R problems escalate.
12. Place of Service (POS) Errors in Orthopedic Claims
Place-of-service denials occur when the billed location does not match where the orthopedic service was actually performed.
These issues commonly affect office-based procedures, ASC claims, and hospital outpatient billing. Coordinating scheduling, facility billing, and coding workflows is essential for preventing POS-related reimbursement delays.
13. Provider Credentialing and Enrollment Denials in Orthopedics
Credentialing denials happen when the rendering provider is not properly enrolled with the payer or linked to the correct practice location and tax ID.
These denials often increase when new orthopedic providers join the practice. Maintaining accurate payer enrollment records and monitoring effective dates can help prevent unnecessary payment delays.
14. NPI and Taxonomy Mismatch Denials
NPI and taxonomy denials occur when payer records do not match the provider information submitted on the claim.
Even small inconsistencies can trigger recurring billing problems. Keeping provider records standardized across credentialing, enrollment, and billing systems is critical for reducing these avoidable denials.
15. Coordination of Benefits (COB) Denials in Orthopedic Billing
COB denials occur when insurance information is outdated or when the payer believes another plan should be billed first.
These denials are common when patients have multiple insurance plans or recent coverage changes. Verifying primary and secondary insurance information during check-in can help reduce payment delays and secondary billing issues.
Orthopedic Modifier Mistakes That Commonly Trigger Denials
Modifiers are not simply billing add-ons in orthopedic coding. They often determine whether a claim is fully reimbursed, partially paid, or denied altogether.
RT/LT Laterality Errors
Laterality errors frequently trigger orthopedic denials because they are easy for payers to identify. Documentation should consistently support the anatomical side across the operative note, imaging report, diagnosis coding, and claim submission.
Distinct Procedural Service Modifier Issues
When billing distinct procedural services, the documentation must clearly demonstrate why the procedures qualify as separate. Different anatomical sites, separate sessions, or clinically distinct encounters should be documented explicitly rather than implied.
Bilateral Procedure Billing Errors
Orthopedic practices frequently bill bilateral procedures and multiple services on the same date. Without standardized coding rules, reimbursement reductions and modifier-related denials become much more common.
E/M With Procedure Denials
E/M visits billed alongside procedures are heavily scrutinized by payers. The documentation must clearly show that the evaluation and medical decision-making went beyond the standard work included with the procedure itself.
Global Period and Post-Operative Billing Rules in Orthopedics
Global period issues are among the most expensive denial drivers in orthopedic billing because they create recurring reimbursement delays that often go unnoticed until A/R begins to grow.
Routine post-operative visits are generally included in the surgical package and are not separately payable. Problems arise when practices bill follow-up visits or additional services without verifying whether they qualify for separate reimbursement.
To reduce these denials, orthopedic practices should:
- Verify the global period before billing post-op services
- Confirm whether the visit qualifies for separate reimbursement
- Document unrelated conditions or separate medical decision-making clearly
- Train providers to avoid generic “routine post-op” documentation when separate billing applies
The goal is not to bill more aggressively. The goal is to bill accurately and defensibly so claims are not trapped in avoidable payer edits.
Documentation Checklist to Reduce Orthopedic Claim Denials
Strong orthopedic documentation should support both clinical care and payer reimbursement requirements. Incomplete documentation remains one of the leading causes of medical necessity denials in orthopedic billing.
A payer-ready orthopedic note should include:
- Clear laterality and anatomical specificity
- Functional limitations and symptom severity
- Objective findings and imaging support
- Conservative treatment history when required
- Procedure rationale and treatment planning
- Diagnosis-to-procedure linkage
- Detailed operative documentation when applicable
Practices that treat documentation as part of the revenue cycle, not a separate clinical task, are far more successful at reducing denials.
A Simple Orthopedic Denial-Prevention Workflow
Denial reduction is not just a billing department responsibility. It requires coordinated workflows across scheduling, coding, documentation, claim submission, and follow-up.
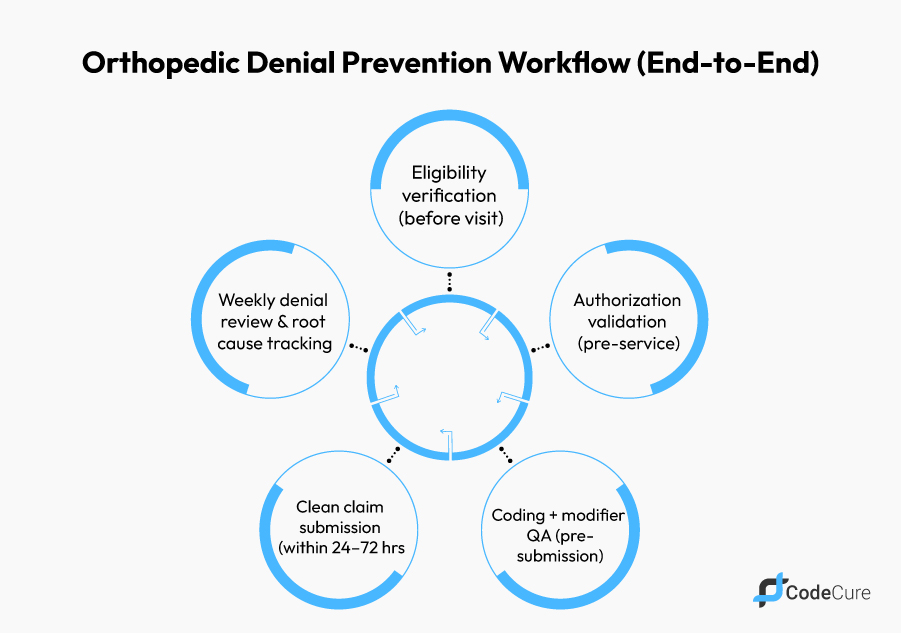
Step 1: Front-End Verification
Before the patient is seen, practices should verify eligibility, confirm referral requirements, validate authorizations, and communicate estimated patient responsibility when appropriate.
Step 2: Orthopedic Coding and Documentation QA
Coding teams should validate diagnosis-to-procedure alignment, confirm laterality and modifiers, review bundling edits, and verify global period impacts before claims are finalized.
Step 3: Clean Claim Submission
Claims should be submitted promptly with ongoing monitoring of payer acknowledgements and clearinghouse responses. Rejections should be corrected immediately to avoid unnecessary delays.
Step 4: Weekly Denial Management and Root-Cause Review
Denials should be reviewed weekly and categorized by root cause, including eligibility, authorization, coding, documentation, enrollment, or COB issues.
Practices that treat denials as operational signals rather than isolated billing events are far more successful at improving long-term revenue cycle performance.
When to Outsource Orthopedic Billing and Coding
Outsourcing orthopedic billing can deliver a strong ROI when internal teams are overloaded or when denial patterns continue repeating month after month.
A strong orthopedic billing partner should be able to:
- Demonstrate orthopedic coding expertise
- Provide denial analytics and root-cause reporting
- Improve authorization and clean-claim workflows
- Reduce A/R aging through measurable process improvements
- Maintain compliance and audit readiness
Questions worth asking include:
- How do you reduce modifier-related denials?
- What does your denial reporting process look like?
- How do you manage global period billing controls?
- How do you monitor provider enrollment accuracy by payer?
How CodeCure Helps Orthopedic Practices Reduce Denials
Denials rarely improve simply by “working harder.” They improve when practices strengthen the workflows that impact claims before submission.
CodeCure helps orthopedic practices reduce denials through coding-first clean-claim QA, authorization validation, modifier and laterality review, medical necessity documentation support, and denial analytics that identify recurring payer and provider trends.
The goal is not just faster follow-up. The goal is building a repeatable orthopedic revenue cycle workflow that reduces denials, improves reimbursement predictability, and prevents A/R from aging into long-term collections problems.
Conclusion
Orthopedic billing denials are not random, and they are not simply “the cost of doing business.” Most denials are caused by repeatable workflow breakdowns involving authorizations, modifier logic, documentation gaps, global period conflicts, enrollment mismatches, or front-end intake errors.
If your orthopedic practice is seeing rising denials, delayed reimbursements, or A/R aging beyond 60–90 days, the most expensive decision is waiting for the problem to correct itself.
The fastest path to stronger cash flow is improving front-end verification, strengthening coding QA, tightening documentation workflows, and treating denials as root-cause signals rather than endless resubmission tasks.
Ready to reduce denials and stabilize collections? CodeCure can help identify where orthopedic revenue is leaking and build a more reliable reimbursement workflow around it.
FAQs
How long do we have to appeal an orthopedic claim denial?
Appeal windows vary by payer and plan, but many allow 30–180 days from the denial date. The practical best practice is to work denials weekly and treat appeals as time-sensitive: submit the first-level appeal (or corrected claim, if that’s the right path) as soon as documentation is complete, and always follow the payer’s appeal hierarchy and formatting requirements.
Should we submit a corrected claim or file an appeal?
Use a corrected claim when the denial is caused by something you can fix on the claim itself (wrong modifier, wrong diagnosis pointer, missing information, units, place of service, rendering/billing mismatch). Use an appeal when the claim is coded correctly, but the payer is disputing medical necessity, policy interpretation, bundling logic, or authorization validation and you need clinical documentation to support payment.
What documentation do payers typically request for orthopedic medical necessity?
Most requests can be satisfied faster when the record clearly shows laterality, symptom severity, functional limitations, objective findings (exam and relevant imaging results), conservative treatment history (when required), and the clinical rationale linking the diagnosis to the service performed. For procedures, include the procedure note/op note elements that support code selection and any modifier rationale.
Why are we getting denials for “included in surgical package” during the global period?
Global period denials usually happen when post-op services are billed as separately payable without verifying global rules or without documentation that supports separate billing. The fix is a consistent workflow: verify global period status before posting charges, confirm the service meets separate-billing criteria per payer policy, and document the medical decision-making and clinical context clearly.
What are the most common modifier-related denial triggers in orthopedics?
The highest-risk issues are laterality (RT/LT) mismatches, unsupported “distinct service” scenarios, multi-procedure logic errors, and E/M billed alongside procedures without documentation that supports separate evaluation/decision-making. Modifier accuracy is one of the fastest levers for reducing repeat denials in orthopedic claims.
What KPIs should an orthopedic practice track weekly to catch denials early?
Track denial rate (by payer and reason), clean-claim rate, days in A/R, % of A/R over 60/90 days, and appeal overturn rate. Reviewing these weekly, especially denial reason trends, helps you fix upstream defects before they become a month-end surprise.


